

Homeopathy and Complementary Integrative Medicine, Dietary and Lifestyle Advices to Reduce Adverse-Effects of Anti-Cancer Therapy: A Cohort Study with Breast Cancer Patients
Elio Rossi 1,*![]() , Cristina Noberasco 1
, Cristina Noberasco 1![]() , Marco Picchi 1
, Marco Picchi 1![]() , Mariella Di Stefano 1
, Mariella Di Stefano 1![]() , Linda Nurra 1
, Linda Nurra 1![]() , Antonella Rossi 1
, Antonella Rossi 1![]() , Leonardo Ventura 2
, Leonardo Ventura 2![]()
- Homeopathic Clinic, Campo di Marte Hospital, Local Health Unit Tuscany North West, Lucca, Italy
- Oncological Network, Prevention and Research Institute – ISPRO, Firenze, Italy
* Correspondence: Elio Rossi![]()
Received: March 28, 2018 | Accepted: August 20, 2018 | Published: September 4, 2018
OBM Integrative and Complementary Medicine 2018, Volume 3, Issue 3 doi:10.21926/obm.icm.1803017
Academic Editor: Michael Frass
Special Issue: Application of Homeopathy in Oncology Patients
Recommended citation: Rossi E, Noberasco C, Picchi M, Stefano MD, Nurra L, Rossi A, Ventura L. Homeopathy and Complementary Integrative Medicine, Dietary and Lifestyle Advices to Reduce Adverse-Effects of Anti-Cancer Therapy: A Cohort Study with Breast Cancer Patients . OBM Integrative and Complementary Medicine 2018;3(3):017; doi:10.21926/obm.icm.1803017.
© 2018 by the authors. This is an open access article distributed under the conditions of the Creative Commons by Attribution License, which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is correctly cited.
Abstract
Background: To manage the adverse effects of anti-cancer treatment, the Homeopathic Clinic of Lucca collaborated with the oncology department of the the Health Unit Toscana North West Lucca and set up an Integrative Oncology Outpatient Unit in the Public Hospital Campo di Marte. Aim: The purpose of this study was to present the results of the homeopathic and complementary integrative medicine treatment targeted at reducing the adverse effects of anti-cancer therapy and cancer symptoms, and to give dietary and lifestyle guidance to improve the quality of life of breast cancer patients. Methods: This is a retrospective observational study conducted on 204 breast cancer patients (all females except 1 male) that consecutively visited the clinic from September 2013 to December 2017, with a mean age of 54.8 (35-88) years. The intensity of symptoms was evaluated according to a graded system as follows: G0 (absence of symptoms), G1 (slight), G2 (moderate), and G3 (strong), as evaluated by the patient in conjunction with the doctor during the course of the visits. The severity of radiodermatitis was evaluated with the Radiation Therapy Oncology Group (RTOG) scale. Homeopathy was the main prescribed therapy; botanicals, acupuncture, and dietary advices were also provided. Results: The most frequently treated symptoms were the adverse effects due to anti-cancer therapies (84.3%), such as endocrine therapy (36.3%), chemotherapy (33.3%), radiotherapy (9.8%), and surgery (4.9%). The treated symptoms caused by cancer were 25.5% and symptoms caused by comorbidities were 21.6%. A comparison of clinical conditions before and after treatment revealed a significant amelioration of the following symptoms: hot flashes (p < 0.01), nausea (p < 0.01), fatigue (p < 0.01), anxiety (p < 0.05), depression (p < 0.01), insomnia (p < 0.01), mucositis (p < 0.01), and joint pain (p < 0.01). The severity of radiodermatitis from radiotherapy was significantly lower in 17 consecutive patients with a homeopathic integrative protocol compared with a control group of 13 patients without treatment. Conclusion: An integrative oncology clinic offers an opportunity to reduce adverse effects of anti-cancer therapy and to improve cancer patients’ quality of life.
Keywords
Homeopathy; integrative oncology; breast cancer patients; complementary integrative medicine; diet
1. Introduction
Breast cancer is the most common cancer among women and has the highest mortality of any cancer in women worldwide [1]. It is the most frequent cancer in European women with an estimated incidence of 494,100 in 2012 [2]; according to American Cancer Society there will be 268,670 new cases of breast cancer (with 41,400 deaths) in the USA in 2018 [3].
Although chemotherapy (CT), radiotherapy (RT), and endocrine and hormonal (HT) therapies are effective against breast cancer [4], they are associated with varied side effects including vasomotor syndrome (occurring in up to 80% of patients), nausea and vomiting (75%), post-mastectomy lymphedema (30-60%), arthralgia (over 40%), neutropenia, cachexia, fatigue, pain, hair loss, hot flashes, and psychological stress [5].
It is for this reason that complementary and integrative medicine (CIM) is frequently used among cancer patients with an estimated use by 45% of patients across different treatment stages [6,7].
The Healthcare Directorate of the Region of Tuscany decided to investigate the use of CIM, since such a large number of cancer patients were utilizing the methods.
1.1 The Tuscan Experience of Integration of Homeopathy and CIM in Oncology
In 2009, the Tuscan Tumor Institute, now ISPRO (www.ittumori.it), and the Tuscan Network of Integrative Medicine (TNIM), now Tuscan Regional Centre for Integrative Medicine, brought together a group of experts in CIM as well as oncologists in order to analyze the international literature on the use of CIM in the treatment of the side effects of anti-cancer therapies and to improve the quality of life of cancer patients. With this as its starting point, the Region of Tuscany authorized and initially funded public clinics in integrative oncology (IO) in the hospitals of Lucca, Florence, Florence Careggi, Pisa, and Grosseto.
At the same time, the TNIM participated in the European Partnership for Action Against Cancer (EPAAC) in the Work Package (WP) “Healthcare” with the aim of collecting evidence on the use of CIM in cancer care and mapping the European centers offering IO services [8]. The EPAAC project ended in March 2014 with the publication of a literature review on the website www.epaac.eu and in a book published in Italian in 2015 [9].
Finally, Tuscan Regional Government Resolution n. 418/2015 was ratified in support of the use of CIM as treatment for cancer-related symptoms and side effects of anti-cancer therapy, such as acupuncture for nausea and post-chemotherapy and post-surgery vomiting, pain, hot flashes in iatrogenic menopause, and xerostomia; homeopathy for hot flashes in iatrogenic menopause and side effects of radiotherapy; and herbal medicine for anxiety, depression, cancer-related fatigue, mucositis, nausea, vomiting, and pain. A commission of CIM experts and oncologists was established to define the modalities of application of the resolution [10].
The Tuscan public hospitals and clinics that currently practice IO are located in Florence (Camerata Clinic and Careggi University Hospital), Lucca, Pisa, Prato, Empoli (Fi), Pitigliano (Gr), and Grosseto.
From September 2013 to September 2016, exactly 2,108 cancer patients consecutively visited the CIM clinics of the public hospitals of Lucca, Florence, Careggi–Florence, Pitigliano, and Pisa [11].
A possible operating model for Tuscan public services attempting to integrate CIM resources into the oncology network is outlined in Figure 1.
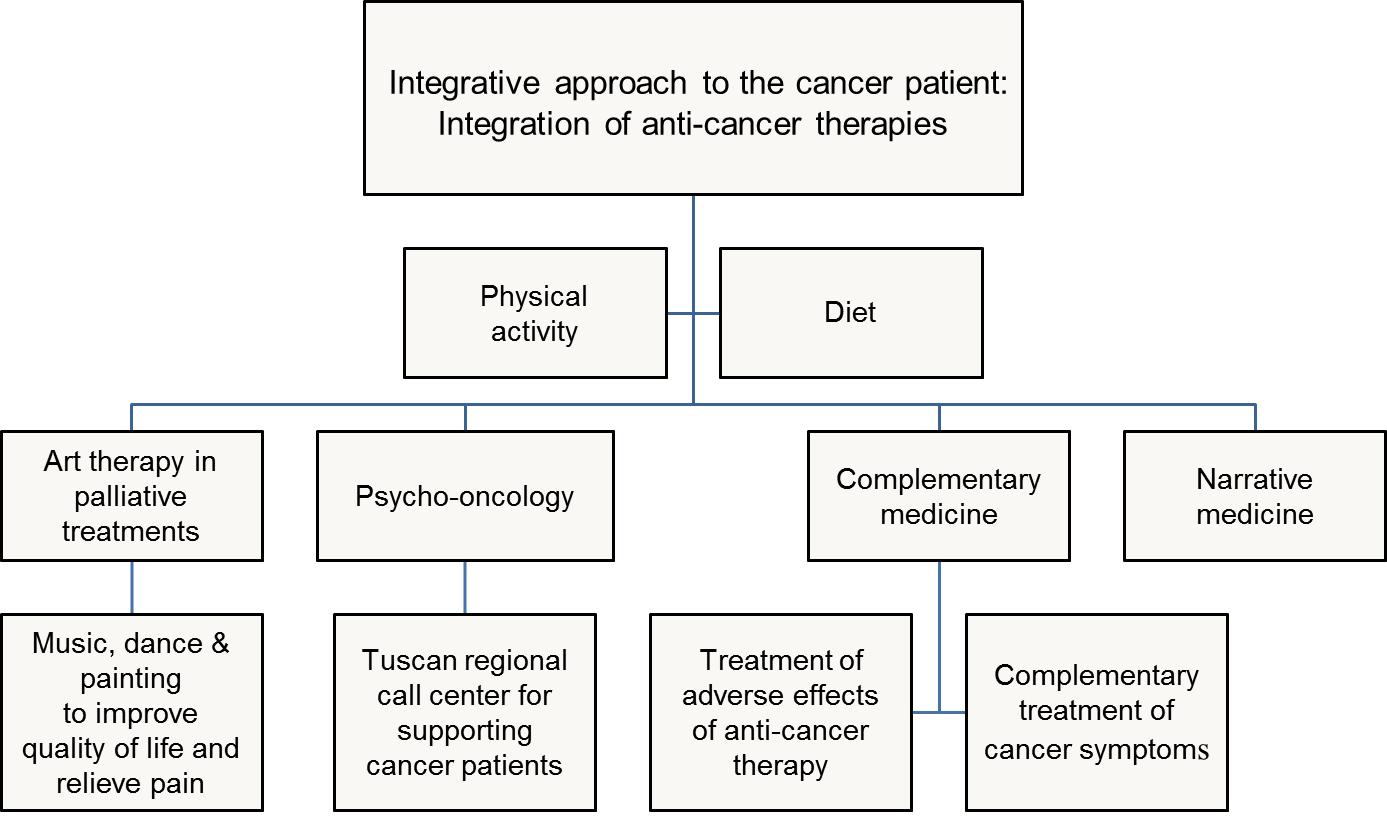
Figure 1 Operating model for an integrative oncology service based on the Tuscan regional experience.
Aim. The aim of this cohort study is to provide general information (sex, age, request for treatment, and type of homeopathic and integrative treatment) and describe the results of using homeopathy and integrative treatments in breast cancer patients (including nutritional recommendations) to reduce the adverse effects of anti-cancer treatment, symptoms of the disease, and to improve the quality of life of breast cancer patients. These observations were made over a 4-year period between 2013 and 2017 at the Clinic of Complementary Medicine and Diet in Oncology of Lucca's public hospital, Campo di Marte (now Cittadella della Salute). Additionally, the severity of radiodermatitis at the end of RT in a group of patients who followed a homeopathic integrative protocol was compared with others who did not follow the protocol.
2. Materials and Methods
2.1 Design
This is a retrospective observational study of a database of 204 consecutive breast cancer patients treated at the Clinic of Complementary Medicine and Diet in Oncology at the Campo di Marte Hospital in Lucca from September 2013 to December 2017.
2.2 Setting
In 2012, the Healthcare Directorate of the region of Tuscany supported [12] a pilot project proposed by the homeopathic clinic of Lucca [13], where CIM would be integrated into the treatment of cancer patients. The project involved setting up an outpatient clinic where the patients from the oncology department of the Hospital of Lucca could meet with both an expert in homeopathy and CIM and an oncologist once a week to receive integrative treatment. The objective was to reduce the adverse effects of anti-cancer treatment and the symptoms of cancer, and to improve patients’ quality of life.
The homeopathic doctor working at the clinic was a professional specialist who attended a homeopathy school for three years, gained over 30 years of experience in the field, and is registered with the Medical Association as an expert in homeopathy, according to Tuscan law n. 9/2007 [14] and the related Agreement Protocol of 2015 [15]. During the medical visit, the CIM physician worked side by side with an oncologist to assess the state of the cancer disease, the prognosis, and the results achieved. Both of them were also experts in herbal therapy, anthroposophic medicine, and Traditional Chinese Medicine.
Since 2015, the Clinic of CM and Diet in Oncology has been officially inserted in the Breast Unit of the Hospital of Lucca. The CIM expert also participates in the meetings organized monthly with women recently diagnosed with breast cancer and the professionals involved in their therapeutic diagnostic path: oncologists, radiotherapists, surgeons, psycho-oncologists, etc.
The patients who wish to be treated with homeopathy and CIM can book an appointment whether they are self-referred or sent by the oncology department of the Local Health Service, Tuscany North West, Lucca. The average waiting times are between one and two weeks. There are no specific eligibility criteria.
2.3 Informed Consent
All of the patients included in this study were asked to sign a privacy disclaimer and an informed consent form for therapy and use of their data for future analyses. As explicitly stated in the written informed consent form, CIM can by no means substitute the anti-cancer treatment prescribed by the referring oncologist. An individual identification number was assigned to all the patients so that the data could be anonymized, collected, and stored in a database.
2.4 Patients
Exhaustive documentation was collected from a sample of 204 patients, 203 (99.5%) of which were females. Only one male was included in our observation. The mean age was 54.8 years. The age group with highest breast cancer incidence was between 50 and 54 years, then 45-49, and then 55-59. Nearly all the patients were referred by their medical oncologists.
The prevalence of patients with breast cancer was mostly due to the high incidence of this pathology, but also to the fact that the Oncology Department of Lucca referring us these patients is a “center of excellence” in the treatment of this type of cancer.
The tumors were not in their initial stage: 6.4% of the patients had a previous history of cancer, 8.3% had a breast cancer recurrence, and 27.9% already had metastases.
2.5 Treatment
At the first examination, the following sociodemographic variables were collected: sex, age, previous conventional or homeopathic treatment, and current state of health, including the severity and nature of the patient’s symptoms. These were recorded in detail according to homeopathic consultation procedures.
Most of the patients were treated with individualized homeopathic treatment (single remedy). However, some patients were treated with combined homeopathic treatment, specific protocols to prepare the patients for RT, CT, or HT, or a combination of both. Conventional drugs or integrative treatments were not excluded and provided when necessary, as described later in this subsection.
The homeopathic treatment protocol of the clinic consisted in administering a single remedy. The treatment can consist in a Quinquagintamillesimal dilution (Q potency) [16], generally starting with 6Q in cycles of at least 45 days. Or, it was administered in a single dose of a high dilution according to Hahnemann’s centesimal scale (C), in a “scale of potencies” (200–M–XM), each dose repeated after about two months. Acute cases were usually treated by remedies in centesimal dilutions at low potencies (from 6 to 30 C).
Homeopathy was the first choice of treatment but homeopathic drugs were sometimes prescribed together with botanicals or other types of food supplements [17] as integrative forms of treatment, which will be described later in the text.
The blood levels of vitamin D were checked for all the patients and if necessary, an integration of this vitamin in the current treatment was proposed, until the correct level was achieved [18,19].
Integrative complementary treatment at the clinic utilized different therapies in addition to the homeopathic remedies. This included botanicals and other kinds of food supplements, as well as acupuncture, sometimes with specific integrative protocols to prepare patients for radiotherapy (RT), chemotherapy (CT), and endocrine therapy (ET).
The most frequently prescribed botanicals were Curcuma longa, employed as detoxifier and antioxidant [20]; bee pollen to reduce and limit hot flashes from iatrogenic menopause, despite the lack of estrogenic activity [21]; indole-3-carbinol produced by the breakdown of glucosinolate glucobrassicin contained in cruciferous vegetables such as broccoli, cabbage, cauliflower, brussels sprouts, collard greens, and kale, which is a chemopreventive and anti-cancer agent [22]; sulphorafane for cancer chemoprevention [23]; green tea (Camellia sinensis L.), known for its antiproliferative, antimutagenic, antioxidant, antibacterial, antiviral, and chemopreventive effects [24]; and ginger (Zingiber officinale Roscoe) to reduce acute chemotherapy-induced nausea [25]. Finally, other types of supplements such as Deuterium sulfate were used in cancer-related fatigue [26]. Viscum album, which has been used in anthroposophic medicine for at least 70 years and now has a sufficient base of clinical evidence [27], was only prescribed occasionally.
Food supplements and botanicals were generally prescribed as dry extract with standardized and titrated active ingredients. In other cases, mother tinctures (hydro-alcoholic extracts) and glycerin macerates (gemmotherapy) were also used.
All of the cancer patients were provided with dietary advice; in addition, psychological counseling and acupuncture were also occasionally recommended in specific cases (5.4%) like those mentioned above.
Patients who requested acupuncture were referred to the acupuncture clinic of the same hospital, which is a clinic for pain control through acupuncture. In addition, patients with pain not well-controlled by conventional and integrative treatments were sent to acupuncture surgery, as well as those who had symptoms of iatrogenic menopause and did not respond to integrative treatment with homeopathy and herbal medicine.
2.6 Dietary Advice
Cancer patients examined at the clinic in Lucca were given practical advice on diet and lifestyle based on data from literature, to combat the progress of cancer and improve their clinical condition and quality of life [20,28]. Primarily, patients were advised to eliminate or reduce the following: refined carbohydrates, in particular white sugar and white flour to lower the glycemic load and consequently blood insulin; red meat, including cured meats to reduce the stimulus of chronic inflammation; harmful substances, such as abuse of alcoholic drinks, tobacco, etc.; and foods for which there is documented food intolerance. The consumption of small-size and oily fish (preferably wild-caught) such as mackerels, anchovies, sardines, and mullets was strongly recommended, as well as the consumption of spices like curcuma, pepper, and ginger. Organic bread, whole grain pasta, spelt, kamut, amaranth, quinoa, brown rice, and whole foods in general were strongly encouraged, and also useful to promote intestinal motility. Small quantities of red wine (preferably organic and without sulfites) was permitted, but no more than 1 glass per day [29].
A very important recommendation for breast cancer patients is the consumption of cruciferous vegetables (cabbage, broccoli, brussels sprouts, etc.) due to their antioxidant properties. Foods containing lignans (anti-estrogenic activity) were also recommended, such as seeds, flax, sesame oil, nuts, and some types of fruit including strawberries and apricots [30]. Foods containing ellagic acid (mixed berries like raspberries, blackberries, and currants) and also pomegranates seem to inhibit cancer angiogenesis [31].
Finally, all cancer patients were advised, if possible, to practice at least 40 minutes of daily physical activity [32].
2.7 Outcome Parameters
In this study, we considered the data from the first and the most recent visit. We collected the symptoms reported by the patient and other types of useful information (e.g. diet, exercise, and style of life).
The intensity of symptoms was evaluated according to a graded system as follows: G0 (Absence of symptoms), G1 (Slight), G2 (Moderate), or G3 (Strong), determined by the patient in agreement with the physician during the visit. For each symptom, we hypothesized the most probable cause (cancer treatment, concomitant effect, the cancer itself, etc.).
In regards to radiodermatitis, we also categorized the total number of RT sessions into 4 groups (“to be started”, “from 1 to 9”, “from 10 to 19”, and “from 20 to 29”). For each patient we recorded personal data (age and sex), clinical data (cancer recurrence, presence of metastasis, localization of cancer, kind of cancer therapy, and possible reasons for not taking a therapy including patient’s refusal), and the kind of homeopathic treatment, herbal treatment, or the combination of both treatments. The group of patients undergoing RT without integrative treatment used only keratoplastic ointments as standard care to promote tissue repair and healing.
The severity of radiodermatitis was evaluated according to the Radiation Therapy Oncology Group (RTOG) scale: G1 indicates toxicity that corresponds to a light and/or painless erythema, epilation, desquamation and/or dryness; G2 indicates sensitive and/or intense erythema, desquamation, partial sweating and/or moderate edema; G3 indicates desquamation, widespread sweating and/or marked edema; G4 indicates ulceration, hemorrhage, or necrosis [33].
2.8 Statistical Analysis
Data entry, screening, encoding, and data analysis were performed by well-trained staff at the homeopathic clinic. Statistical analyses were performed using the statistical software package PASW (release 18.1 of SPSS, Statistical Package for Social Sciences). Outcome evaluation of the main symptoms was conducted via Wilcoxon’s test applied to matched-pair samples, associated with a two-tailed significance test.
3. Results
From September 2013 to December 2017, 204 breast cancer patients were consecutively examined at the Clinic of Complementary Medicine and Diet in Oncology of the Campo di Marte Hospital in Lucca. During these 4 years of activity, 113 patients (55.4% of the total) had at least one follow-up visit.
Table 1 describes the requests for treatment due to the effects of anti-cancer therapies received by breast cancer patients attending the CM clinic of Lucca. Most patients had a form of CT, alone or combined with other antineoplastic therapies; however, the most frequent therapies were endocrine therapy and radiotherapy. As a result, the most requested interventions were relative to the adverse effects of anti-cancer treatment: 172 patients (84.3%), plus three patients requesting treatment for the adverse effects of other conventional therapies (corticosteroids and statins), followed by the request for treatment of cancer symptoms (52 patients or 25.5%) and from the comorbidities (44 or 21.6%). Only one patient had no ongoing treatment.
Table 1 Effects of anticancer therapies received by 204 breast cancer patients.

Table 2 lists the symptoms reported by the patients after conventional anti-cancer therapy. As expected, hot flashes (46.3%) and articular pain (11.6%) that are connected to endocrine therapy were the most frequently observed symptoms; lymphedema was mainly related to surgery (4%) and radiodermatitis(19%) to radiotherapy. There was a strong request for the treatment of depression (20.3%) and anxiety (15.3%) due to the course of the cancer disease. Asthenia/fatigue, nausea, and vomiting were the main side effects of CT (23.9%).
Table 2 Main symptoms supposedly subsequent to conventional anti-cancer treatment presented by breast cancer patients treated with CIM.
Table 3 shows the effects of the complementary treatment applied to the different symptoms presented by breast cancer patients. Analysis of the outcomes of the treatment was performed without the availability of a control group. Therefore, we compared the intensity of the symptoms performed on a graded scale from G0 to G3, as reported in Materials and Methods. The graded value was determined at the time of the first visit and then compared with the value given by the patient during their most recent follow-up visit. By comparing the clinical conditions before and after the CIM treatment, we observed a significant improving, as evidenced by Wilcoxon’s test for paired samples for the most frequently observed symptoms: hot flashes (p < 0.01), nausea (p < 0.01), fatigue (p = 0.001), anxiety (p < 0.05), depression (p < 0.01), insomnia (p < 0.01), mucositis (p < 0.01), joint pain (p < 0.01), and totality of symptoms (p < 0.01).
Table 3 Effectiveness of homeopathic and CIM treatment on the symptoms more frequently presented by breast cancer patients.
One issue that arose was that of the disturbances associated with RT treatment where the RT therapy worsens symptoms, such as radiodermatitisin the final stage of the RT series. In this case, the patient usually came to the clinic when RT was ongoing or in its early stage. The effects of preventive treatment were then evaluated.
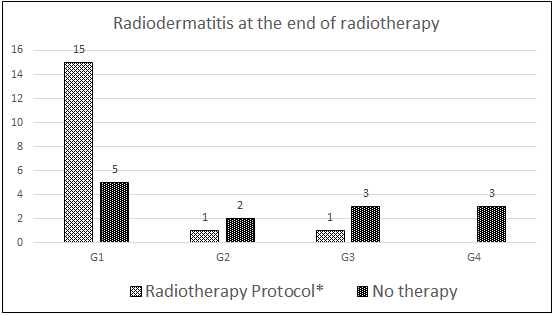
The severity of radiodermatitisin a group of 30 consecutive breast cancer patients undergoing RT was evaluated at the beginning and at the end of the treatment; 17 patients with a homeopathic integrative protocol during RT were compared with a control group of 13 patients without treatment. Preliminary results showed that 15 patients with integrative treatment had G1, 1 patient had G2, and 1 had G3 toxicity; in the group of patients who did not follow the treatment, 5 patients had G1, 2 patients had G2, 3 patients had G3, and finally 3 patients had G4 toxicity. The Mann-Whitney U test yielded a two-tailed significance of p ≤ 0.01. (Fig. 2)
Figure 2 Severity of radiodermatitis at the end of the cycle of radiotherapy in 17 patients with the homeopathic/integrative protocol and in 13 patients of the control group (Total patients =30).
|
G1 |
G2 |
G3 |
G4 |
Tot. |
|
|
Radiotherapy Protocol |
15* |
1** |
1 |
- |
17 |
|
No therapy |
5 |
2 |
3 |
3 |
13 |
|
Total |
20 |
3 |
4 |
3 |
30 |
Mann-Whitney U test: two-tailed significance p ≤ 0.01
* 2 patients with G1 at the end had respectively G3 and G0 when the protocol was started.
** 1 patient with G2 at the end had G3 when the radiotherapy protocol was started.
A percentage of breast cancer patients refused (9 patients or 4.4%) or decided to discontinue conventional anti-cancer treatment (3 patients) against the advice of their oncologists. All of these patients were women with mean age of 56.3 years; five of these patients (23.8%) had a previous history of cancer, two (9.5%) had a cancer recurrence, and nine of them (42.8%) already had metastases. Of these patients, eight (70%) refused chemotherapy and four (30%) refused or discontinued endocrine therapy. At present, five patients (41.7%) have died, while the others are in good condition; after the integrative oncology visit, 4 out of 12 (30%) patients agreed to undergo standard oncological treatments.
Additionally, we investigated the types of homeopathic treatment used in the integrated form of treatment, namely homeopathic treatment combined with botanicals (48.5%), or the prescription of homeopathy treatment alone (51.5%). In some situations, when the more striking, singular, and characteristic symptoms of the case were either missing or insufficient [26], the Banerji Protocol was applied [27]. In other cases, simple but also specific protocols were suggested in order to prevent the adverse effects of radiotherapy, chemotherapy, and surgery. The rationale of this therapeutic proposal is that the symptoms appearing in the patient after CT or RT treatment are often similar because the toxic effects of the anti-cancer substances are also similar.
Differences were observed in the percentage of therapeutic success between the uses of exclusive homeopathy (68.1%) and homeopathy integrated with other therapies (76.6%). However, there were no differences in the therapeutic success of the various integrative treatments: homeopathy and acupuncture had a therapeutic success of 81.8%, homeopathy and herbal medicine had a therapeutic success of 80.0%, and homeopathy and other treatments had a therapeutic success of 80.0%. Integrative treatments (homeopathy and acupuncture, homeopathy and herbal medicine, and homeopathy and others) were used more frequently to treat the following symptoms: hot flashes, articular pain, asthenia, insomnia, liver steatosis, and weight gain. The effect of exclusive versus integrated homeopathic therapy was compared with the most frequently treated symptoms (hot flashes, articular pain, asthenia, nausea, insomnia, and depression), but there were no significant differences in outcomes.
Furthermore, in patients who reported and wanted to address weight gain, the diet worked in 66.7% of cases; there was no significant difference between those who combined the diet with supplements and those who did not use them.
Finally, Table 4 presents the most frequently prescribed forms of treatment, including both homeopathic and botanical remedies, as well as other therapies that were utilized in addition to homeopathy, which remained the primary therapy. The most common homeopathic remedies prescribed were Lachesis mutus, Phosphorus, and Nux vomica. Lachesis mutus is the most common remedy among patients in artificial menopause induced by endocrine therapy (treated with Tamoxifene and aromatase inhibitors), Phosphorus is likely the most useful remedy against the adverse effects of anti-cancer therapies, and Nux vomica is the most common remedy to treat digestive symptoms.
Table 4 Complementary integrative treatments used to reduce adverse effects of anti-cancer therapy in breast cancer patients.
4. Bias
This study reports on the clinical activity carried out since 2013. It was not possible to compare the results of CIM treatment in cancer patients with those of a control group. In the future, it will be necessary to document the efficacy of IO with randomized and controlled trials, ideally compared with a placebo.
Another potential bias is the fact that a general and non-specific method of evaluation was used to calculate outcomes, without using specific scales of symptoms evaluation; however, more specific criteria were used to evaluate the severity of the symptoms of radiodermatitis [33], which was also compared with the outcomes of a non-randomized control group.
5. Discussion
Breast cancer is the most common female cancer in Western countries and there is substantial appeal from cancer patients to integrate conventional anti-cancer treatment with complementary medicines [1]. This appeal is especially of interest to those in advanced stages of the disease who may be treated with a large variety of chemo-endocrine therapeutic agents and the increasing development of a multitude of target therapies, in order to enhance their quality of life and long-term survival. The complexity of this disease and its treatment offers clinicians the possibility to integrate different approaches to optimize side effect management; reduce stress, anxiety, and pain; and to improve the quality of life.
According to the experience of integrative oncology in our clinic, the patients who were treated with complementary and integrative medicine did not seem to have a specific psychological profile. In the great majority of cases (at least 80%), they were patients who were referred by the oncology department of the hospital because the patients had concern with some of the conventional anti-cancer treatments and the concerns could possibly be mollified by CIM treatment, in the opinion of oncologists.
The decision by policy makers and public health authorities such as those in Tuscany to offer their citizens the opportunity to use complementary and integrative products and practices designed to promote well-being is a good step for integrative health.
The results of this study, although limited due to the lack of a control group and of a specific symptoms assessment test, suggest that homeopathy and other integrative therapies may be effective in reducing cancer symptoms and anti-cancer treatment side effects. This reduction was especially observed in the intensity and frequency of hot flashes, insomnia, and mood instability resulting from endocrine therapy that causes a premature iatrogenic menopause in young females or increases these symptoms already present in post-menopausal women. With the exception of the Hormone Replacement Therapy (HRT) and soy supplements which are both contraindicated, there are no truly effective therapies to alleviate these symptoms. Therefore, homeopathic therapy, which is commonly integrated with other natural treatments such as bee pollens [21] and other botanicals or acupuncture [36], can fill a conventional therapeutic void. However till now, isotherapeutic treatments are not routinely prescribed as suggested by other experiences [37].
Our results confirmed that homeopathy and CIM in cancer care are mainly used in treatment or in prevention to reduce adverse effects of hormone therapy (36.3%) and chemo-radiotherapy (33.3%). In addition, patients’ requests are related to the need to decrease tumor-related symptoms (25.5%) such as fatigue, anxiety, and depression.
According to our data there is a significant increasing effect on the quality of life of integrated treatments, particularly homeopathy plus herbal medicine with or without acupuncture, compared to the use of homeopathy as an exclusive therapy.
These treatments seem to increase the effectiveness of homeopathic treatment without interfering with the action of homeopathy. Finally, the results are similar for every type of treatment applied.
Frass M. and his colleagues came to the same conclusions (2015) in a pragmatic randomized controlled trial that studied the global health status and subjective well-being of 410 patients treated by standard anti-neoplastic therapy. The patients were randomized to receive or not to receive classical homeopathic adjunctive therapy in addition to standard therapy. The improvement of global health status between visits 1 and 3 was significantly stronger in the homeopathy group by 7.7 (95% CI 2.3–13.0; p = 0.005) when compared with the control group. A significant group difference was also observed with respect to subjective well-being by 14.7 (95% CI 8.5–21.0; p < 0.001) in favor of the homeopathic group as compared with the control group [38].
In addition to this, a prospective observational study by Rostock M. and his colleagues observed a statistically significant improvement in quality of life of cancer patients under complementary homeopathic treatment in the first three months of treatment and a subsequent increase after 12 months of treatment. A decrease in fatigue symptoms in cancer patients was also observed [39].
A certain percentage of patients (21.6%) also chose natural therapies because they are non-toxic and non-invasive for controlling concomitant symptoms or disturbances not related to cancer disease. In some cases, these are patients already using homeopathy or complementary therapies in their daily life who do not want to alter their behavior even while being treated for cancer. In other cases, it was a specific choice to reduce new side effects resulting from other additional drugs and to prevent an overload on the liver, kidneys, and other organs.
It is noteworthy to mention the results of homeopathic and integrative therapy in regards to the prevention of skin damage caused by radiotherapy, as documented in the literature [40,41]. The application of a simple therapeutic protocol based on the administration of the homeopathic remedy Radium bromatum before RT, followed by either Belladonna or by other specific remedies (Radium bromatum or Apis mellifica), has shown significant effects in reducing skin inflammation from RT retrospectively compared to patients who did not receive the protocol. Although further studies are necessary to confirm this data, these preliminary outcomes are very promising, especially considering the economic sustainability of the treatment proposed and the relative ease of application.
Lastly, an interesting aspect emerged from the analysis of the data that involves patients (about 6%) coming to the visit with the intention of either refusing or suspending conventional anti-cancer treatment against the advice of their oncologist, and requesting an “alternative” therapy for their disease. The presence of CIM experts in a comprehensive breast cancer service, as recognized by the Breast Cancer Specialist Guidelines of Eusoma [42], can encourage these patients to reconsider the possible serious consequences deriving from a do-it-yourself approach or from the advice of non-professional figures, including the Internet or word of mouth. After the interview with the CIM physician, around 30% of these patients accepted to follow the anti-cancer treatment. Although it is a small percentage, it is relevant as these types of patients are skeptical towards conventional therapies and the dialogue with them is often difficult.
Integrative oncology can strengthen the collaboration with referring oncologists and at the same time allow the cancer patients to be supported in such a critical phase of the disease potentially increasing their quality and duration of their lives.
6. Conclusion
The integration of evidence-based complementary treatments in conventional cancer care allows medical doctors and healthcare professionals to respond more effectively to the demand coming from cancer patients to reduce many side effects of anti-cancer therapies, as well as to improve their quality of life offering both safety and equal access in public healthcare systems.
In this process of integration, exchanging knowledge and experiences is fundamental. It is therefore necessary for physicians (primarily oncologists) and other healthcare professionals in the cancer field to be appropriately informed about the potential benefits of complementary and integrative medicines.
Acknowledgements
We would like to thank Drs. Lucia Tanganelli, Oncology Department; Stefania Tocchini and Lucia Da Valle, Psychology Department; Aroldo Marconi, Breast Unit of Lucca hospital, for their precious collaboration to the clinical activities. We also thank Dr. Laura Cignoni for the English
translation of this article.
Author Contributions
All research done by the authors. Elio Rossi carried out clinical activities, conceived, designed,participated in the research and wrote the article; Cristina Noberasco carried out clinical activities,participated in the research and wrote the article; Marco Picchi participated in the analysis of data and the writing of the article; Mariella Di Stefano participated in the writing and discussion of the article; Linda Nurra participated in data analysis and the writing of the article; Antonella Rossi contributed to updating the literature on use of botanicals, Leonardo Ventura for statistical analysis.
Competing Interests
No conflict of interest. All the costs of this study were supported by the Public Health System of the Tuscany Region.
References
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C. et al. Cancer Incidence and Mortality Worldwide: IARC Cancer. Base No. 11 [Internet]. Lyon, France: International Agency for Research on Cancer; 2013. Available at: http://globocan.iarc.fr.
- Curado MP, Edwards B, Shin HR, Storm H, Ferlay J, Heanue M et al. Cancer Incidence in Five Continents, Vol. IX. Lyon: IARC Scientific Publications No. 160; 2007. [Google scholar]
- Breast [Internet]. American Cancer Society, Cancer Statistics Center; 2018 [cited date (2018 February 26)]. Available from: https://cancerstatisticscenter.cancer.org/#!/cancer-site/Breast.
- Senkus E, Kyriakides S, Ohno S, Penault-Llorca F, Poortmans P. Rutgers E. et al. Primary breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015; 2: v8-v30. [CrossRef] [Google scholar] [PubMed]
- U.S. Department Of Health And Human Services. Common Terminology Criteria for Adverse Events (CTCAE). Version 5.0. 2017 [cited date (2017 November 27)]. Available from: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf.
- Konkimalla VB, Efferth T. Evidence-based Chinese medicine for cancer therapy. J Ethnopharmacology. 2008; 116: 207-210. [CrossRef] [Google scholar] [PubMed]
- Di Gianni LM, Garber JE, Winer EP. Complementary and alternative medicine use among women with breast cancer. J Clin Oncol. 2002; 20: 34S-8S. [Google scholar]
- Rossi E, Vita A, Baccetti S, Di Stefano M, Voller F, Zanobini A. Complementary and alternative medicine for cancer patients: results of the EPAAC survey on integrative oncology centres in Europe. Support Care Cancer. 2014. DOI 10.1007/s00520-014-2517-4. [CrossRef] [Google scholar] [PubMed]
- Baccetti S, Di Stefano M, Rossi E. Le medicine complementari per il paziente oncologico. Sviluppo e opportunità dell’oncologia integrata. Felici Ed. Pisa, 2015. [Google scholar]
- Region of Tuscany. Delibera n. 418 del 07-0-2015. Integrazione delle medicine complementari nella Rete oncologica dell'Istituto Toscano Tumori. Available from: http://www.regione.toscana.it/bancadati/atti/.
- Rossi E, Baccetti S, Picchi M, Conti T, Firenzuoli F, Guido C, et al. Complementary medicine in oncology: a multicenter retrospective study on 1928 patients with cancer in the Region of Tuscan (Italy). BMC Complement Altern Med. 2017; 17: 133. [Google scholar]
- Region of Tuscany. Delibera n. 405 del 15-05-2012. Struttura di riferimento regionale per le Medicine Complementari: programma attività, trasferimento Struttura di riferimento per la Fitoterapia e destinazione risorse fondo finalizzato regionale MC, anno 2012. Available from: http://www.regione.toscana.it/bancadati/atti/Contenuto.xml?id=222726&nomeFile=Delibera_n.405_del_14-05-2012-Allegato-A.
- Delibera Giunta Regionale Toscana N. 1163 del 28-12-2010. Destinazione fondo finalizzato all'integrazione delle medicine complementari negli interventi per la salute: anno 2010. Available from: http://www301.regione.toscana.it/bancadati/atti/Contenuto.xml?id=104671&nomeFile=Delibera_n.1163_del_28-12-2010.
- Tuscany Region Regional Law no. 9/2007. Available from: http://jtest.ittig.cnr.it/cocoon/regioneToscana/xhtml?doc=/db/nir/RegioneToscana/2007/urn_nir_regione.toscana_legge_2007–02–19n9&css=&datafine=20121214 (Accessed on 5th march 2018)
- Tuscany Region Practice of complementary medicine by Medical Doctors and Dentists, Veterinaries and Pharmacists. Agreement Protocol of R.L. n.9/2007. Available at: http://www.regione.toscana.it/documents/10180/70874/Delibera%2049_08/98fe234d-6212-4013-99d0-4d1d6e51e7bd.
- De Schepper L. LM potencies: one of the hidden treasures of the Sixth edition of the Organon. Br Homeopath J. 1999; 88: 128-134. [CrossRef] [Google scholar] [PubMed]
- Frenkel M, Abrams DI, Ladas EJ, Deng G, Hardy M, Capodice JL, et al. Integrating Dietary Supplements into Cancer Care. Integr Cancer Ther. 2013; 12: 369-384. [CrossRef] [Google scholar] [PubMed]
- Deuster E, Jeschke U, Ye Y, Mahner S, Czogalla B. Vitamin D and VDR in gynecological cancers-A systematic review. Int J Mol Sci. 2017; 18: E2328. [CrossRef] [Google scholar] [PubMed]
- Oliveira Sediyama CM, Dias MM, Pessoa MC, Queiroz AR, Suhett LG, Freitas RN, et al. Lifestyle and vitamin D dosage in women with breast cancer. Nutr Hosp. 2016; 33: 584. [CrossRef] [Google scholar] [PubMed]
- Bruno E, Gargano G, Villarini A, Traina A, Johansson H, Mano MP, et al. Adherence to WCRF/AICR cancer prevention recommendations and metabolic syndrome in breast cancer patients. Int J Cancer. 2016; 138: 237-44. [CrossRef] [Google scholar] [PubMed]
- Villarini A, Pasanisi P, Traina A, Mano MP, Bonanni B, Panico S, et al. Lifestyle and breast cancer recurrence: the DIANA-5 trial. Tumori. 2012; 98: 1-18. [CrossRef] [Google scholar] [PubMed]
- Touillaud MS, Thiébaut ACM, Fournier A, Niravong M, Boutron-Ruault MC, Clavel-Chapelon F. Dietary lignan intake and postmenopausal breast cancer risk by estrogen and progesterone receptor status. J Natl Cancer Inst. 2007; 99: 475-486. [CrossRef] [Google scholar] [PubMed]
- Zhang HM, Zhao L, Li H, Xu H, Chen WW, Tao L. Research progress on the anticarcinogenic actions and mechanisms of ellagic acid. Cancer Biol Med. 2014; 11: 92-100. [Google scholar]
- Lemanne D, Cassileth B, Gubili J. The role of physical activity in cancer prevention, treatment, recovery, and survivorship. Oncology 2013; 27: 580-585. [Google scholar] [PubMed]
- Cox JD, Stetz J, Pajak TF. Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC). Int J Radiat Oncol Biol Phys. 1995; 31: 1341-1346. [CrossRef] [Google scholar] [PubMed]
- Hahnemann S. Organon of medicine. 5th Edition. New Delhi: B Jain Publisher; 1983. p. 217-218. [Google scholar]
- Prasanta Banerji, Pratip Banerji. A Compendium of Essays on Alternative Therapy. 2012. p. 123-144. Available from: http://cdn.intechopen.com/pdfs/26491.pdf.
- Shanmugam MK, Rane G, Kanchi MM, et al. The multifaceted role of curcumin in cancer prevention and treatment. Molecules. 2015; 20: 2728-2769. [CrossRef] [Google scholar] [PubMed]
- Munstedt K, Voss B, Kullmer U. Bee pollen and honey for the alleviation of hot flushes and other menopausal symptoms in breast cancer patimenti. Mol Clin Oncol. 2015; 3: 869-874. [CrossRef] [Google scholar] [PubMed]
- Weng JR, Tsai CH, Kulp SK, Chenc CS. Indole-3-carbinol as a chemopreventive and anti-cancer agent. Cancer Lett. 2008; 262: 153. [CrossRef] [Google scholar] [PubMed]
- Tortorella SM, Royce SG, Licciardi PV, Karagiannis TC. Dietary sulforaphane in cancer chemoprevention: The role of epigenetic regulation and HDAC inhibition. Antioxid Redox Signal. 2015; 22: 1382-1424. [CrossRef] [Google scholar] [PubMed]
- Li MJ, Yin YC, Wang J, Jiang YF. Green tea compounds in breast cancer prevention and treatment. World J Clin Oncol. 2014; 5: 520-528. [CrossRef] [Google scholar] [PubMed]
- Ryan JL, Heckler CE, Roscoe JA., Dakhil SR., Kirshner J, Flynn PJ, Hickok JT, Morrow GR. Ginger (Zingiber officinale) reduces acute chemotherapy-induced nausea: A URCC CCOP study of 576 patients. Support Care Cancer. 2012; 20: 1479-1489. [CrossRef] [Google scholar] [PubMed]
- Catalani S, Carbonaro V, Palma F, et al. Metabolism modifications and apoptosis induction after Cellfood™ administration to leukemia cell lines. J Exp Clin Cancer Res. 2013; 32: 63. [CrossRef] [Google scholar] [PubMed]
- Kienle, GS, Kiene H. Review article: Influence of Viscum album L. (European mistletoe) extracts on quality of life in cancer patients: A systematic review of controlled clinical studies. Integr. Cancer Ther 2010; 9: 142-157. [CrossRef] [Google scholar] [PubMed]
- Befus D, Coeytaux RR, Goldstein KM, McDuffie JR, Shepherd-Banigan M, Goode AP, et al. Management of menopause symptoms with acupuncture: An umbrella systematic review and meta-analysis. J Altern Complement Med. 2018; 24: 314-323. [CrossRef] [Google scholar] [PubMed]
- Bagot JL. Using hetero-isotherapics in cancer supportive care: the fruit of fifteen years of experience. Homeopathy. 2016; 105: 119-125. [CrossRef] [Google scholar] [PubMed]
- Frass M, Friehs H, Thallinger C, Sohal NK, Marosi C, Muchitsch I, et al. Influence of adjunctive classical homeopathy on global health status and subjective wellbeing in cancer patients - A pragmatic randomized controlled trial. Complement Ther Med. 2015; 23: 309-317. [CrossRef] [Google scholar] [PubMed]
- Rostock M1, Naumann J, Guethlin C, Guenther L, Bartsch HH, Walach H. Classical homeopathy in the treatment of cancer patients--a prospective observational study of two independent cohorts. BMC Cancer. 2011; 17: 19. [Google scholar]
- Balzarini A, Felisi E, Martini A, De Conno F. Efficacy of homeopathic treatment of skin reactions during radiotherapy for breast cancer: a randomized, double-blind clinical trial. Br Homeopath J. 2000; 89: 8-12. [CrossRef] [Google scholar] [PubMed]
- Pommier P, Gomez F, Sunyach MP, D’Hombres A, Carrie C, Montbarbon X. Phase III randomized trial of Calendula officinalis compared with trolamine for the prevention of acute dermatitis during irradiation for breast cancer. J Clin Oncol. 2004; 22: 1447-1453. [CrossRef] [Google scholar] [PubMed]
- Baum M, Ernst E, Lejeune S, Horneber M. Role of complementary and alternative medicine in the care of patients with breast cancer: report of the European Society of Mastology (EUSOMA) Workshop, Florence, Italy, December 2004. Eur J Cancer. 2006; 42: 1702-1710. [CrossRef] [Google scholar] [PubMed]
