

Emotional Freedom Techniques for Food Cravings in Overweight Adults: A Comparison of Treatment Length
Peta Stapleton 1,* ![]() , Hannah Chatwin 1
, Hannah Chatwin 1 ![]()
- School of Psychology, Bond University, Queensland, Australia
* Correspondence: Peta Stapleton![]()
Received: May 17, 2018 | Accepted: June 25, 2018 | Published: July 3, 2018
OBM Integrative and Complementary Medicine 2018, Volume 3, Issue 3 doi:10.21926/obm.icm.1803014
Academic Editor: Gerhard Litscher
Recommended citation: Stapleton P, Chatwin H. Emotional Freedom Techniques for Food Cravings in Overweight Adults: A Comparison of Treatment Length. OBM Integrative and Complementary Medicine 2018;3(3):014; doi:10.21926/obm.icm.1803014.
© 2018 by the authors. This is an open access article distributed under the conditions of the Creative Commons by Attribution License, which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is correctly cited.
Abstract
(1) Background: Because patients vary in their response to treatment, including adherence, the effect of treatment length in the use of EFT on food cravings was examined by comparing two studies in order to ascertain if shorter programs are as effective. This may then impact treatment adherence and completion. (2) Methods: In study one, 96 overweight and obese adults were randomly allocated to a 4-week treatment for their food craving or waitlist condition. In study two, an 8-week EFT program for 47 adults, the same variables were measured as per study one. Participants were assessed for degree of food craving, perceived power of food, restraint capabilities and psychological symptoms at pre-, post-, 6- and 12-month follow-up. (3) Results: Outcomes indicated significant reductions in food cravings, subjective power of food, dietary restraint, Body Mass Index, and weight for both interventions. There were no significant differences between the intervention groups in terms of the effect size of outcomes for the variables measured, thus indicating that the 4-week EFT treatment could achieve the outcomes that the 8-week program did. (4) Conclusions: While the efficacy of EFT as an adjunct to standard dietary and exercise programs has been established through several clinical trials, it has not been clear as to the optimal length of program required to achieve successful results. This comparison of a brief 4-week (8-hour) program versus an 8-week (16-hour program) indicated significant reductions in all measures for both intervention lengths. Length of treatment may be important when considering adherence and motivation.
Keywords
Emotional Freedom Techniques; brief therapy; weight loss; food cravings; obese; adults; Tapping
1. Introduction
Food cravings are thought to be an important intervening causal variable in the development of extreme eating behaviours, and in turn, obesity [1,2,3]. Research suggests consistent dieting results in short- to medium-term weight loss [4]. Moreover, meta-analytic studies indicate that the more time that elapses between the end of a diet and the follow-up period, the more weight that is regained [5]. Weight cycling and instability has been associated with poorer perceptions of health and wellbeing [6], excess body weight and abdominal fat accumulation [7], lower health satisfaction and self-esteem, higher body dissatisfaction, and binge eating, for both men and women [7]. Unfortunately, dieting alone does not lead to sustained weight loss, and individuals who diet sporadically are more likely to gain back more weight than they lost [5].
Behavioural strategies such as self-control, restricted food choices and engaging in frequent and strenuous physical activity have been cited as necessary for successful weight loss and maintenance [8,9,10] however people also benefit from psychological interventions to enhance weight reduction [11]. Cognitive-Behaviour Therapy (CBT), Behavior Therapy, relaxation therapy, and hypnotherapy have all been indicated as beneficial in improving weight loss [11]. More recently, Energy Psychology (EP) strategies have emerged as techniques which can improve emotional, behavioural, and cognitive concerns by combining physical interventions with a cognitive element [12,13,14,15].
Emotional Freedom Techniques (EFT) [16,17] is an exposure therapy approach that includes a somatic component. In addition, it has a cognitive element and is designed to target the stress response and has been researched for a variety of psychological problems. The EFT technique involves a participant rating a level of distress or concern on a scale of zero to 10 (0 being no distress, and 10 indicating the most distress), and then stating that problem in a cognitive statement, which includes an acceptance ending (e.g., “Even though I have this food craving, I accept myself”). The subject then taps with two fingers on acupressure points on the face and body as they continue to state a shortened reminder phrase of their problem (see Figure 1 for the acupressure points). This is considered a ‘round’ of tapping and after each round; the subject continues to re-rate their level of distress.
The stress hyperarousal response includes activation of the amygdala, and recent studies of the use of EFT have indicated a decrease in amygdala and hippocampus activity [18]. The mechanism of EFT may include this impact on physiological systems in the body that regulate stress and anxiety [19]. Functional magnetic resonance imaging (fMRI) and positron emission tomography (PET) scan investigations of neurological shifts following acupoint stimulation consistently produced prominent decreases of activation in the amygdala, hippocampus, and other brain areas associated with fear and pain [20,21,22]. EFT also results in a number of biomarker changes, including stress hormones [23], gene expression [15,23], electroencephalogram (EEG) activity [24,25], and fMRI-detected brain activation patterns [26]. Finally, EFT has also been found to be an “evidence-based” practice for anxiety, depression, phobias and PTSD when measured against the standards of the American Psychological Association’s Division 12 Task Force on Empirically Validated Treatments [14].
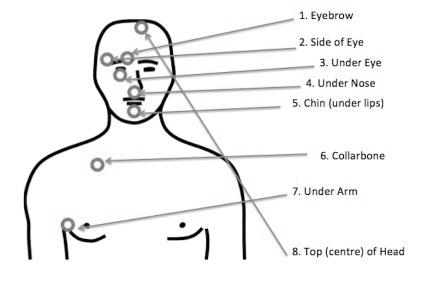
Figure 1 EFT Points.
1.1 Main Text
EFT has now had 43 randomized controlled trials and 39 outcome studies published indicating a range of positive outcomes for conditions such as post traumatic stress disorder [27,28,29,30], generalized and specific anxiety, phobias, depression [31], and chronic pain [32]. A meta-analysis for anxiety disorders has found the pre-post effect size for the EFT treatment group was 1.23 (95% CI: 0.82-1.64, p < 0.001), while the effect size for combined controls was 0.41 (0.17-0.67, p = 0.001) [33]. A systematic review and meta-analysis of both randomised and non-randomised trials for the treatment of PTSD in veterans demonstrated a large treatment effect size (d = 2.96) when comparing EFT to treatment as usual or a wait-list conditions [34]. Another meta-analysis has indicated EFT treatment results in a large effect size(d = 1.31) for the treatment of depression [35]. This is of particular interest because a number of studies have noted an association between depression and weight loss, and obesity has been considered to cause or exacerbate depressive symptoms [36]. Depression symptoms have been noted as improving after successful weight loss with EFT [37].
EFT reuslts in significant changes in a range of variables related to weight. Over the course of a one-day EFT workshop for a group of 216 healthcare workers a significant reduction in cravings for a range of food substances, alcohol and tobacco from the beginning of the day to post-intervention at the end of the day [38].
Significant improvements in weight, body mass index, craving intensity, subjective power of food, craving restraint and psychological coping occur with EFT, and lasts over 12-months [39]. When compared to a gold standard treatment such as CBT, EFT has been found to be non-inferior in areas related to dietary restraint and food cravings. Cohen’s effect size values of EFT are moderate to high [40]. This suggested that EFT was comparable to a gold standard, thus offering more evidence based options to clients.
1.2 The Present Study
The current comparison of previously collected data from two randomized clinical EFT trials, aimed to ascertain whether a 4-week treatment was as effective as an 8-week treatment. It was anticipated this may have future implications for more time-efficient treatment delivery.
Ethics Statement
Ethical approval was obtained for the current study from the lead author’s affiliated university at the time, and both studies were registered under the Australia New Zealand Clinical Trials Registry.
2. Materials and Methods
2.1 Recruitment
Two previous randomized clinical trials offered EFT for food cravings to overweight and obese adults [39,40]. One trial was a 4-week group program, of two hours a week, resulting in eight hours of treatment. The other was an 8-week group program, of two hours a week, resulting in 16 hours of treatment.
Ethical approval was obtained for the current study from the lead author’s affiliated university at the time, and both studies were registered under the Australia New Zealand Clinical Trials Registry. Male and female participants were originally recruited through community announcements in print advertisements, radio, and television. In order to be eligble for inclusion, participants had to be over 18 years, have frequent food cravings,) a Body Mass Index greater than 25 to fit the overweight defintion, and not engaged in any other treatment (psychological or medical) for their food cravings. The studies excluded known sufferers of diabetes (Type I and II) and hypoglycaemia, as well as women who were pregnant, as there was the potential for food cravings to be affected by these variables. Sufferers of anorexia nervosa were also excluded.
2.2 Participants
In the 4-week trial, 96 adults completed the treatment, and in the 8-week trial, 47 participants completed the treatment. All participants completed the outcome measures below at pre- and post- and 6- and 12-month follow-up periods to ascertain effectiveness of the EFT treatment over time.
4-week group participants. The majority of participants in the 4-week group were female (89.0%), over 40 years of age (68.0%), married (53.1%), did not live alone (87.0%), had undertaken some form of education since high school (60.0%), were employed (79.0%) and had a household income exceeding 50, 000 (65.0%).
8-week group participants. Participants in the 8-week group were female (88%), over 40 years of age (54%), married (48%), had undertaken some form of education since high school (51%), were employed (59%) and had a household income exceeding 50, 000 (46%).
2.3 Intervention
The lead author and an independent certified EFT practitioner developed and reviewed the treatment manuals to ensure that the active ingredients of the EFT intervention were fully operationalized as per Church [17]. While the preferred approach to assess adherence to the delivery of the EFT program would have been to use audio and video recording, privacy of the participants was paramount and this methodology was not chosen. Instead, treatment fidelity checklists were used. The same qualified EFT practitioner delivered both programs, with the assistance of a support therapist (i.e., psychologist) present in each session. Treatment was delivered as group therapy with 10 to 15 participants in each group, and sessions involved direct exposure to craved foods while the participants engaged in the EFT process.
All participants chose one food to address in their treatment group from the following list of groups: chocolate, salty carbohydrate foods,sweet carbohydrate foods,carbohydrate foods which are neither sweet nor salty such as white refined foods,and caffeinated products.
2.4 Outcome Measures
All eligible participants were asked to complete a demographic questionnaire, the Food Craving Inventory (FCI) [41], the Power of Food Scale (POF) [42], and the Revised Restraint Scale (RRS) [39].They also self reported height and weight measurements and the researchers then calculated each BMI, which was defined as weight in kilograms divided by height in meters squared (kg/m²). The BMI categories utilised were: underweight (< 18.5), healthy weight (18.5 to 24.9), overweight (25.0 to 29.9), or obese (≥ 30.0).
Food Craving Inventory. The FCI is a reliable and valid measure for the assessment of cravings for specific types of foods: High Fats, Sweets, Carbohydrates/Starches, and Fast Food Fats. These individual foods impact the higher order construct of “food craving”, and this is considered to be the FCI Total score [41]. A higher score for each of the subscales reflect stronger cravings for that food type with the range being 0 to 185. The FCI is a valid and psychometrically sound instrument for general and specific food cravings, with good internal consistencies ranging from .70 (fast food) to .91 (high fats) for the subscales and .86 to .87 for the total scale [41,44]. It also has adequate temporal stability and discriminant validity, and good sensitivity to changes across treatment.
Power of Food Scale. The POF scale is a 21-item scale assesess the psychological influence of the mere presence of food. High scores on the POF scale indicate greater responsiveness to an individual’s food environment. The POF scale has been shown to be valid and sound with studies demonstrating adequate internal consistency, temporal stability, and convergent validity [42,45].
The Revised Restraint Scale. The RRS is a vliad and sound measure and consists of two subscales which are weight fluctuation and concern with dieting. All items are scored on a four- to five-point Likert scale, with a maximum total score of 35. Higher scores indicate chronic dieting, including constant cycling on and off a diet/s without substantial weight loss. Restrained eating is defined as a score of 16 or greater in females, and 12 or greater in males. High dietary restraint is a contributer to eating disorder development, obesity, and loss of control over food intake [46,47,48,49].
3. Results
The data were analysed using SPSS (Version 22) using an alpha level of .05.
3.1 Preliminary Analyses
Chi-square analyses were performed to examine whether the two intervention groups (96 adults in the 4-week trial, and 47 adults in the 8-week trial) differed based on demographic variables. Results of these analyses revealed no significant differences between groups in relation to gender χ2(1) = .17, p = .680; marital status χ2(5) = 2.17, p = .25; age χ2(8) = 6.80, p = .250; education level χ2(7) = 13.51, p = .061; income χ2(10) = 51.841, p = .100; or employment area χ2(19) = 25.79, p = .136.
3.2 Main Analyses
A mixed (between-within subjects) 2 x 5 MANOVA was conducted to determine whether the different intervention lengths (4 weeks vs 8 weeks) influenced the dependent variables (e.g., FCI, POF, RRS, weight, and BMI) combined, over time (pre-intervention vs post-intervention vs 6-month follow-up vs 12-month follow-up). A non-significant Box’s M indicated the homogeneity of variance-covariance matrix assumption had not been violated. Mauchly's Test of Sphericity for each of the dependent variables indicated the assumption of sphericity had been violated, therefore Huynh Feldt was utilised in order to determine if the test was statistically significant.
With the use of Wilk’s criterion, a significant multivariate main effect was found for Time F(15, 26) = 6.83, p = < .001, partial η2 = .80, power = 1.00. Findings revealed there was no significant main effect for Intervention Length (p = .749), and no significant interaction between Time and Intervention Length (p = .205). Therefore, further analyses will be focused primarily on the main effect of Time.
Given the significant multivariate main effect, univariate analysis of variance (ANOVAs) for each dependent variable was assessed.
Food craving. Univariate analyses revealed a significant main effect of Time on the FCI F(2.33, 93.12) = 13.39, p = < .001, partial η2 = .25, power = 1.00. Simple effects analyses for Time revealed significant differences in FCI scores across time were elicited for the four-week intervention group, F(3.00, 39.00) = 7.37, p = .001, η2 = .36, power = .98. Pairwise comparisons with Sidak adjustment revealed FCI scores decreased significantly from pre-intervention to post-intervention for four-week intervention group participants with this reduction maintained at 12-month follow-up, but not 6-month follow-up. For the eight-week intervention group, significant differences in FCI scores were also seen F(2.06, 55.72) = 7.75, p = .001, η2 = .22, power = 0.94. Pairwise comparisons with Sidak adjustment revealed FCI scores decreased significantly from pre-intervention to post-intervention for eight-week intervention group participants, with this reduction maintained at 6-month follow-up and 12-month follow-up (see Table 1).
Power of food. Univariate analyses revealed a significant main effect of Time on the POF F(2.18, 87.24) = 27.31, p = < .001, partial η2 = .41, power = 1.00. Simple effects analyses for Time revealed significant differences in POF scores were elicited for the four-week intervention group over time, F(3.00, 39.00) = 29.14, p = < .001, η2 = .69, power = .87.43. Pairwise comparisons with Sidak adjustment revealed POF scores decreased significantly from pre-intervention to post-intervention for four-week intervention group participants with this reduction maintained at 6-month, and 12-month follow-up points. For the eight-week intervention group, significant differences in POF scores were also observed, F(2.06, 55.63) = 9.84, p = < .001, η2 = .28, power = 0.98. Pairwise comparisons with Sidak adjustment revealed POF scores decreased significantly from pre-intervention to post-intervention for eight-week intervention group participants, with this reduction maintained at 6-month follow-up and 12-month follow-up.
Restraint. Univariate analyses revealed a significant main effect of Time on the RRS F(2.12, 78.54) = 11.46, p = .002, partial η2 = .14, power = 0.92. Simple effects analyses for Time revealed significant differences in restraint scores were elicited for the four-week intervention group over time F(3.00, 39.00) = 2.94, p = .045, η2 = .19, power = .65. However, pairwise comparisons with Sidak adjustment revealed no statistically significant changes in restraint scores from pre-intervention to post-intervention 6-month follow-up, or 12-month follow-up. For the eight-week intervention group, significant differences in restraint scores were also seen F(1.85, 49.96) = 9.55, p < .001, η2 = .26, power = .97. Pairwise comparisons with Sidak adjustment revealed restraint scores did not decrease significantly from pre-intervention to post-intervention, or from pre-intervention to 6-month follow-up. However, post-hoc tests revealed a statistically significant decrease in restraint scores from pre-intervention to 12-month follow-up, indicating a delayed effect of the EFT-based treatment for the eight-week intervention group.
BMI. Simple effects analyses for Time revealed significant differences in BMI scores were elicited for the four-week intervention group over time F(2.01, 26.08) = 5.11, p = .013, η2 = .28, power = .78. However, pairwise comparisons with Sidak adjustment revealed no statistically significant changes in BMI scores from pre-intervention to post-intervention, 6-month follow-up, or 12-month follow-up. For the eight-week intervention group, no statistically significant differences in BMI scores was observed across any time points.
Weight. Simple effects analyses for Time revealed significant differences in weight scores were elicited for the four-week intervention group over time F(2.19, 28.51) = 4.71, p = .014, η2 = .27, power = .78. However, pairwise comparisons with Sidak adjustment revealed no statistically significant changes in weight scores from pre-intervention to post-intervention, 6-month follow-up, or 12-month follow-up. For the eight-week intervention group, no statistically significant differences in weight scores was observed across any time point.
See Table 1.
Table 1 Means and standard deviations for dependent variables as a function of group and time.
|
Variable |
|
4-Week Intervention Group (n = 14) |
|
|
8-Week Intervention Group (n = 28) |
|
||
|
n |
M |
SD |
p |
n |
M |
SD |
p |
|
|
FCI (Baseline) |
98 |
62.21 |
16.80 |
|
49 |
61.68 |
20.52 |
|
|
POF (Baseline) |
98 |
76.86 |
15.63 |
|
49 |
70.43 |
21.31 |
|
|
RRS (Baseline) |
98 |
32.07 |
4.65 |
|
49 |
33.18 |
6.28 |
|
|
Weight (Baseline) |
98 |
95.21 |
16.41 |
|
49 |
94.13 |
28.80 |
|
|
BMI (Baseline) |
98 |
33.00 |
5.42 |
.154 |
49 |
33.44 |
7.19 |
|
|
FCI (Post) |
98 |
45.93 |
15.36 |
.013* |
49 |
48.58 |
13.65 |
.016* |
|
POF (Post) |
98 |
51.36 |
18.63 |
<.001* |
49 |
53.32 |
21.37 |
.001* |
|
RRS (Post) |
96 |
30.07 |
5.58 |
.741 |
49 |
31.50 |
5.61 |
.121 |
|
Weight (Post) |
98 |
94.43 |
16.26 |
.755 |
49 |
90.43 |
20.45 |
|
|
BMI (Post) |
98 |
32.57 |
5.79 |
.575 |
49 |
33.07 |
7.17 |
|
|
FCI (6-mth follow-up) |
49 |
48.79 |
12.26 |
.065 |
27 |
48.39 |
12.33 |
.021* |
|
POF (6-mth follow-up) |
49 |
41.71 |
12.36 |
<.001* |
27 |
49.39 |
27.06 |
.001* |
|
RRS (6-mth follow-up) |
49 |
27.50 |
6.27 |
.158 |
28 |
28.50 |
9.37 |
.072 |
|
Weight (6-mth follow-up) |
48 |
91.86 |
14.22 |
.590 |
28 |
89.59 |
25.19 |
|
|
BMI (6-mth follow-up) |
48 |
31.79 |
4.84 |
|
28 |
33.87 |
15.25 |
|
|
FCI (12-mth follow-up) |
46 |
46.00 |
15.24 |
.003* |
27 |
51.75 |
14.43 |
.022* |
|
POF (12-mth follow-up) |
46 |
46.93 |
14.69 |
<.001* |
28 |
51.29 |
22.86 |
.002* |
|
RRS (12-mth follow-up) |
46 |
29.93 |
5.46 |
.689 |
28 |
24.07 |
11.84 |
.004* |
|
Weight (12-mth follow-up) |
48 |
87.57 |
14.73 |
.065 |
28 |
89.68 |
25.25 |
.497 |
|
BMI (12-mth follow-up) |
48 |
29.86 |
4.62 |
.058 |
28 |
33.88 |
15.36 |
.803 |
*p<.005
4. Discussion
The current paper compared the outcomes of a 4-week EFT treatment versus an 8-week EFT treatment, over time. The aim was to ascertain if treatment length had an impact on outcome measures, in order to potentially affect adherence rates for clients.
Overall, findings indicated significant reductions in food cravings, subjective power of food, dietary restraint, BMI, and weight for both intervention lengths. The lack of statistically significant interaction effect and main effect of intervention length indicates that there was no significant difference between the intervention groups, in terms of the variables measured. Ultimately, the findings imply that a briefer, 4-week EFT intervention achieves comparable results to a longer, 8-week EFT program.
Further analyses did indicate some differences between the intervention lengths that are worth noting. For food cravings, the 8-week intervention produced effects that were maintained at 6- and 12-month follow-up, while the four-week intervention did not maintain this effect at 6-months. The longer length of this program may have resulted in improved cravings and is worthy of note in programs moving forward. For restraint, the 8-week intervention produced effects that were maintained at all measured time points, while the four-week intervention produced an overall effect but no specific effect between time points. Again, the additional treatment sessions in the 8-week program influenced restraint ability above and beyond the briefer program, and is also recommended for future programs. Previous EFT for weight loss studies [39] have indicated that restraint often takes longer to respond (only becoming significant at the 6-month point), which may be a function of the measure used, or the decreases in other variables (e.g. food craving severity) assisted internal regulation over time.
Finally, for BMI and weight, the four-week intervention produced an overall effect while the eight-week intervention did not. The four-week intervention actually resulted in more weight loss (eight kilograms over 12 months versus five kilograms for the longer program), and we suspected that adherence was better for the shorter length. This was not an expected outcome given the longer length program resulted in better outcomes in food craving severity and restraint ability and thus it was expected to see greater weight loss. It must be mentioned that neither program included any dietary or exercise advice, which may have impacted total weight loss. While the participants in the 8-week program did lose weight and this was clinically significant, it may have been that the more concise and succinct program resulted in better adherence and attendance. A larger sample size would potentially impact this variable and is highly recommended.
The program was evaluated weekly byparticipants. A seven-point Likert scale was used (0 represented ‘not at all’) and 91% of participants in the 4-week program indicated EFT addressed their concerns ‚very well‘, and 89% found the EFT program to ‘very much’ meet their goals for reducing food cravings. In the 8-week intervention, 93% of the participants in the 8-week program indicated EFT addressed their concerns very well, and 88% found the EFT program to ‘very much’ meet their goals for reducing food cravings. Evidently, evaluation ratings indicated that participants’ satisfaction with the EFT program was similarly high across intervention lengths.
4.1 Limitations
The results of this comparison may be understated due to the limitations of sample size and attrition, as is common in longitudinal studies. Due to the nature of the study and its research questions, data was included only if participants had completed all measures at each time point (i.e., pre-intervention, post-intervention, 6-month follow-up, and 12-month follow-up – see Table 1). This then limits the data reported and its generalizability to the wider community.
Caution is also needed when interpreting retrospectively collected data. Future research would benefit from a well designed randomized trial of the two treatment lengths (four-week versus eight-week), including a control condition, before conclusions about treatment length are fully established.
5. Conclusions
While the efficacy of EFT as an adjunct to standard dietary and exercise programs has been established through several clinical trials, it has not been clear as to the optimal length of program required to achieve successful results. This paper presents a comparison of a brief 4-week (8-hour) program versus an 8-week (16-hour program). Overall findings indicated significant reductions in all measures for both intervention lengths. The briefer, 4-week EFT treatment achieved comparable results to a longer, 8-week EFT program, however it is important for future interventions moving forward to consider the impact a longer program can have on maintaining reductions in food craving severity and restraint ability. This may be relevant to participants who have struggled with weight issues for a longer peirod of time. Larger sample clinical trials are recommended to ascertain the long term impact of weight loss after EFT.
Author Contributions
Dr. Stapleton supervised the original trials, and Ms Chatwin assisted with the analysis and writeup of this comparison paper.
Funding
The authors acknowledge the Association for Comprehensive Energy Psychology for supporting the intervention trials with funding.
Competing Interests
The authors have declared that no competing interests exist.
References
- Delahanty LM, Meigs JB, Hayden D, Williamson DA, Nathan DM. Psychological and behavioral correlates of baseline BMI in the diabetes prevention program (DPP). Diabetes Care. 2002; 25, 1992-1998. [CrossRef] [Google scholar] [PubMed]
- Franken IHA, Muris P. Individual differences in reward sensitivity are related to food craving and relative body weight in healthy women. Appetite. 2005; 45, 198-201. [CrossRef] [Google scholar] [PubMed]
- Hill AJ, Heaton-Brown L. The experience of food craving: A prospective investigation in healthy women. J Psychosom Res. 1994; 38: 801-814. [CrossRef] [Google scholar] [PubMed]
- Perri M, Fuller P. Success and failure in the treatment of obesity: Where do we go from here. Med Exerc Nutr Health. 1995; 4: 255-272. [Google scholar]
- Mann T, Tomiyama AJ, Westling E, Lew AM, Samuels B, Chatman J. Medicare's search for effective obesity treatments: diets are not the answer. Am Psychol. 2007; 62: 220. [CrossRef] [Google scholar] [PubMed]
- Foster GD, Sarwer DB, Wadden TA. Psychological effects of weight cycling in obese persons: A review and research agenda. Obes Res. 2012; 5: 474-488. [CrossRef] [Google scholar] [PubMed]
- Cereda E, Malavazos AE, Caccialanza R, Rondanelli M, Fatati G, Barichella M. Weight cycling is associated with body weight excess and abdominal fat accumulation: A cross-sectional study. Clin Nutr. 2011; 30: 718-723. [CrossRef] [Google scholar] [PubMed]
- Hill JO, Wyatt H, Phelan S, Wing R. The National Weight Control Registry: is it useful in helping deal with our obesity epidemic? J Nutr Educ Behav. 2005; 37: 206-210. [CrossRef] [Google scholar] [PubMed]
- Raynor HA, Jeffery RW, Phelan S, Hill JO, Wing RR. Amount of food group variety consumed in the diet and long‐term weight loss maintenance. Obes Res. 2012; 13: 883-890. [CrossRef] [Google scholar] [PubMed]
- Wing RR, Hill JO. Successful weight loss maintenance. Annu Rev Nutr. 2001; 21: 323-341. [CrossRef] [Google scholar] [PubMed]
- Shaw K, O'Rourke P, Del Mar C, Kenardy J. Psychological interventions for overweight or obesity. Cochrane Database Syst Rev. 2005; 2: 1-62. [CrossRef] [Google scholar] [PubMed]
- Church D, Feinstein D, Palmer-Hoffman J, Stein PK, Tranguch A. Empirically supported psychological treatments: The challenge of evaluating clinical innovations. J Nerv Ment Dis. 2013; 202: 699-709. [CrossRef] [Google scholar] [PubMed]
- Feinstein D. Energy psychology: A review of the preliminary evidence. Psychotherapy. 2008; 45: 199. [CrossRef] [Google scholar] [PubMed]
- Feinstein D. Acupoint stimulation in treating psychological disorders: Evidence of efficacy. Review of General Psychology. 2012; 16, 364-380. [CrossRef] [Google scholar]
- Maharaj ME. Differential gene expression after Emotional Freedom Techniques (EFT) treatment: A novel pilot protocol for salivary mRNA assessment. Energy Psychol. 2016; 8: 17-32. [Google scholar]
- Craig G. The EFT manual. Fulton, CA: Energy Psychology Press, 2011. [Google scholar]
- Church D. The EFT manual. 3rd ed. Santa Rosa, CA: Energy Psychology Press; 2013. [Google scholar]
- Dhond RP, Kettner N, Napadow V. Neuroimaging acupuncture effects in the human brain. J Altern Complement Med. 2007; 13: 603-616. [CrossRef] [Google scholar] [PubMed]
- Diepold Jr JH, Goldstein DM. Thought field therapy and qEEG changes in the treatment of trauma: A case study. Traumatology. 2009; 15: 85-93. [CrossRef] [Google scholar]
- Fang J, Jin Z, Wang Y, Li K, Kong J, Nixon EE, Hui KK-S. The salient characteristics of the central effects of acupuncture needling: Limbic-paralimbic-neocortical network modulation. Hum Brain Mapp. 2009; 30: 1196-1206. [CrossRef] [Google scholar] [PubMed]
- Hui KKS, Liu J, Marina O, Napadow V, Haselgrove C, Kwong KK, Makris N. The integrated response of the human cerebro-cerebellar and limbic systems to acupuncture stimulation at ST 36 as evidenced by fMRI. NeuroImage. 2005; 27: 479-496. [CrossRef] [Google scholar] [PubMed]
- Napadow V, Kettner N, Liu J, Li M, Kwong KK, Vangel M, Hui KK. Hypothalamus and amygdala response to acupuncture stimuli in carpal tunnel syndrome. Pain. 2007; 130: 254-266. [CrossRef] [Google scholar] [PubMed]
- Church D, Yount G, Brooks AJ. The effect of Emotional Freedom Techniques (EFT) on stress biochemistry: A randomized controlled trial. J Nerv Ment Dis. 2012; 200: 891-896. [CrossRef] [Google scholar] [PubMed]
- Lambrou PT, Pratt GJ, Chevalier G. Physiological and psychological effects of a mind/body therapy on claustrophobia. Subtle Energ Energ Med, 2003; 14: 239-251. [Google scholar]
- Swingle PG, Pulos L, Swingle MK. Neurophysiological indicators of EFT treatment of posttraumatic stress. Subtle Energ Energ Med. 2004; 15: 75-86. [Google scholar]
- Stapleton P. Emotional Freedom Techniques for food cravings and emotional eating. Appl Psychol Health Well Being. 2016; 8: 232-57. [CrossRef] [Google scholar] [PubMed]
- Church D, Hawk C, Brooks A, Toukolehto O, Wren M, Dinter I, Stein P. Psychological trauma symptom improvement in veterans using EFT (Emotional Freedom Techniques): A randomized controlled trial. J Nerv Ment Dis, 2013; 201: 153-160. [CrossRef] [Google scholar] [PubMed]
- Church D, Brooks AJ. CAM and energy psychology techniques remediate PTSD symptoms in veterans and spouses. Explore. 2014; 10: 24-33. [CrossRef] [Google scholar] [PubMed]
- Gallo FP. Energy tapping for trauma: Rapid relief from post-traumatic stress using energy psychology. Oakland, CA: New Harbinger; 2007. [Google scholar]
- Geronilla L, Minewiser L, Mollon P, McWilliams M, Clond M. EFT (Emotional Freedom Techniques) remediates PTSD and psychological symptoms in veterans: A randomized controlled replication trial. Energ Psychol. 2016; 8: 29-41. [CrossRef] [Google scholar]
- Stapleton P, Devine S, Chatwin H, Porter B, Sheldon T. A feasibility study: Emotional freedom techniques for depression in Australian adults. Curr Res Psychol, 2014; 5: 19-33. [CrossRef] [Google scholar]
- Stapleton P, Chatwin H, Shepperd L, McSwan J. The lived experience of chronic pain and the impact of brief Emotional Freedom Techniques (EFT) group therapy on coping. Energ Psychol. 2016; 8: 18-28. [CrossRef] [Google scholar]
- Clond M. Emotional Freedom Techniques for anxiety: A systematic review with meta-analysis. J Nerv Ment Dis. 2016; 204: 388-395. [CrossRef] [Google scholar] [PubMed]
- Sebastian B, Nelms J. The effectiveness of Emotional Freedom Techniques in the treatment of Posttraumatic Stress Disorder: A meta-analysis. Explore. 2017, 13: 16-25. [CrossRef] [Google scholar] [PubMed]
- Nelms J, Castel D. A systematic review and meta-analysis of randomized and non-randomized trials of Emotional Freedom Techniques (EFT) for the treatment of depression. Explore-J Sci Heal. 2016; 12: 416-426. [Google scholar]
- Wing RR, Phelan S. Long-term weight loss maintenance. Am J Clin Nutr. 2005, 82: 222-225. [CrossRef] [Google scholar] [PubMed]
- Stapleton P, Church D, Sheldon T, Porter B, Carlopio C. Depression Symptoms Improve after Successful Weight Loss with Emotional Freedom Techniques. ISRN Psychiatry. 2013: 573532. [CrossRef] [Google scholar] [PubMed]
- Church D, Brooks AJ. The effect of a brief EFT (Emotional Freedom Techniques) self-intervention on anxiety, depression, pain and cravings in healthcare workers. Integr Med Clin J. 2010, 9: 40-44. [Google scholar]
- Stapleton PB, Sheldon T, Porter B, Whitty J. A randomized clinical trial of a meridian-based intervention for food cravings with six-month follow-up. Behav Change. 2011; 28: 1-16. [CrossRef] [Google scholar]
- Stapleton P, Bannatyne A, Porter B, Urzi KC, Sheldon T. Food for Thought: A Randomised Controlled Trial of Emotional Freedom Techniques and Cognitive Behavioural Therapy in the Treatment of Food Cravings. Appl Psychol Health Well Being. 2016; 8: 232-57. [CrossRef] [Google scholar] [PubMed]
- White MA, Whisenhunt BL, Williamson DA, Greenway FL, Netemeyer RG. Development and validation of the Food-Craving Inventory. Obesity. 2002; 10: 107-114. [CrossRef] [Google scholar] [PubMed]
- Lowe MR, Butryn ML, Didie ER, Annunziato RA, Thomas JG, Crerand CE, Halford J. The Power of Food Scale: A new measures of the psychological influence of the food environment. Appetite. 2009; 53: 114-118. [CrossRef] [Google scholar] [PubMed]
- Herman CP, Polivy J. Restrained eating. In A. J. Standard (Ed.), Obesity Philadelphia, PA: W. B. Saunders; 1980. (pp. 208-225). [Google scholar]
- White MA, Grilo C. Psychometric properties of the Food Craving Inventory among obese patients and binge eating disorder. Eat Behav.2005; 6: 239-245. [CrossRef] [Google scholar] [PubMed]
- Cappelleri JC, Bushmakin AG, Gerber RA, Leidy NK, Sexton CC, Karlsson J, Lowe MR. Evaluating the Power of Food Scale in obese subjects and a general sample of individuals: Development and measurement properties. Int J Obes, 2009; 33: 913-922. [CrossRef] [Google scholar] [PubMed]
- Fedoroff IC, Polivy J, Herman CP. The effect of pre-exposure to food cues on the eating behavior of restrained and unrestrained eaters. Appetite. 1997; 28: 33-47. [CrossRef] [Google scholar] [PubMed]
- Overduin J, Jansen A. Food cue reactivity in fasting and non-fasting subjects. Eur Eat Disord Rev. 1996; 4: 249-259. [CrossRef] [Google scholar]
- Davis C, Katzman MA. Chinese men and women in the United States and Hong Kong: Body and self-esteem raings as a prelude to dieting and exercise. Int J Eat Disord. 1998; 23: 99-102. [CrossRef] [Google scholar]
- Klem ML, Klesges RC, Bene CR, Mellon MW. A psychometric study of restraint: The impact of race, gender, weight, and marital status. Addict Behav. 1990; 15: 147-152. [CrossRef] [Google scholar] [PubMed]
